Abstract
Background
Place is a contributor to overall health in the United States. Health disparities exist in relation to spatial variables, and minorities and people who live below the Federal Poverty Level (FPL) experience the greatest burden. Most individuals with sickle cell disease in the U.S. are minorities, signaling an increased likelihood of exposure to the deleterious impact of social determinants of health. Because the impact of social determinants of health outcomes is not well investigated in sickle cell disease, we sought to create a model to investigate the relationship between contextual factors and clinical outcomes. Specifically, we investigated the variability of fetal hemoglobin (HbF) level during hydroxyurea therapy in a longitudinal cohort of patients with sickle cell anemia (SCA). We hypothesized that patients living in neighborhoods with lower Economic Hardship Index (EHI) would have lower HbF in comparison with those living in places with higher EHI scores.
Methods
We included patients with SCA who are participants of the longitudinal natural history study, Sickle Cell Clinical Research and Intervention Program (Hankins et al. Pediatr Blood Cancer. 2018 May 24:e27228.), who 1) lived in Shelby County, Tennessee, 2) were treated with hydroxyurea, and 3) had at least one HbF value recorded. Using ArcGIS, participant addresses were geocoded then aggregated by U.S. Census Block Group (CBG). Geospatial analysis was conducted to identify clustering of HbF values using Cluster and Outlier Analysis (Anselin Local Moran's I), High/Low Clustering (Getis-Ord GeneralG), and Hot Spot Analysis (Getis-Ord Gi*). Geographically-weighted regression was used to test explanatory variables for identified clusters. The main outcome variables were peak, minimum, and average HbF during hydroxyurea therapy at the CBG level. Mean HbF the average of all HbF lab values for the duration of treatment, the peak HbF was recorded at hydroxyurea maximum tolerated dose, and minimum HbF was the lowest record value during treatment. Spatial regression was used to examine factors associated with HbF at the individual level (demographics, genotype, and duration of hydroxyurea therapy).
Results
A total of 202 SCCRIP participants (HbSS N=187; HbSβ0-Thalassemia, N=14; other, N=1) were identified during the years 1996 and 2017. The median age (range: 0.8-25.3 years) was 12 years. Participant addresses were geocoded within 147 (23.4%) of the 628 CBGs within Shelby County. Mean (SD) duration of hydroxyurea therapy was 5.4 (±4.8) person-years, mean, maximum, and minimum HbF was 23.6% (SD±10.8), 52.2% (SD±25.9) and 12.9% (SD±9.7), respectively. Thirty-nine percent of participants lived in a census block group with high to very high EHI scores (i.e., increased economic hardship as measured by U.S. Census data) and 19.3% lived within a CBG where >40% of households fall below the federal poverty level (FPL).
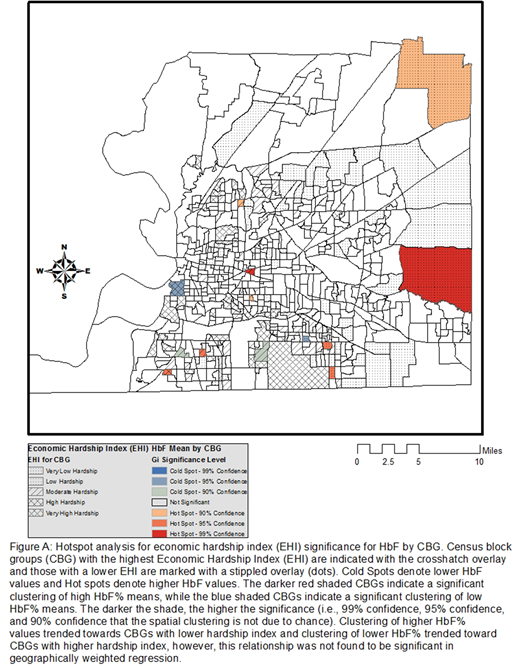
Age was a significant predictor of peak [(F(1,200)=191.34, p<0.001, R2=.489], mean [(F(1,200)=118.99, p<0.001), R2 =0.373], and minimum HbF [(F(1,200)=58.33, p<0.001, R2=.226]. However, mean age was randomly distributed throughout the study area without significant clustering at the CBG level (Observed General G=0.0068, z-score=0.313, p=0.754). Hot Spot Analysis (Getis-Ord Gi*) found significant clustering of HbF values at the CBG level (Figure): higher HbF clustered with CBGs above the FPL and lower HbF clustering with CBGs below the FPL. While there was differential HbF clustering at the CBG level when stratified by EHI, the geographically weighted regression did not find a significant relationship between EHI and HbF levels.
Conclusion
Geospatial analysis indicates geographic variation in HbF% levels among individuals with SCA living in Shelby County, TN. Clustering of higher HbF trended towards neighborhoods with lower EHI while clustering of lower HbF trended toward neighborhoods with higher EHI, suggesting a role of the environment on response to hydroxyurea therapy. Although this study did not investigate the mechanism whereby economic hardship may influence HbF production during hydroxyurea therapy, our findings suggest a possible link between poverty and medication adherence. Our findings point toward the importance of tailoring hydroxyurea therapy to contextual factors, such as neighborhood types, informing community-level interventions.
Estepp:Daiichi Sankyo: Consultancy; NHLBI: Research Funding; ASH Scholar: Research Funding; Global Blood Therapeutics: Consultancy, Research Funding. Hankins:Novartis: Research Funding; Global Blood Therapeutics: Research Funding; bluebird bio: Consultancy; NCQA: Consultancy.